Experiencing ear numbness following facelift surgery is one of the most common yet concerning sensations patients encounter during their recovery journey. This temporary loss of sensation around the auricular region affects the vast majority of individuals who undergo facial rejuvenation procedures, ranging from mild tingling to complete numbness that can persist for several months. Understanding the underlying mechanisms behind this phenomenon helps patients navigate their recovery with realistic expectations and appropriate peace of mind.
The occurrence of post-operative sensory changes stems from the intricate relationship between surgical technique and the complex network of nerves that innervate the face and neck region. During rhytidectomy procedures, surgeons must carefully navigate around numerous sensory pathways whilst achieving optimal aesthetic outcomes. This delicate balance between surgical precision and nerve preservation determines both the extent and duration of any resulting sensory disturbances.
Neuroanatomical basis of Post-Rhytidectomy sensory disturbances
The human face and neck contain an intricate network of sensory nerves that provide tactile sensation, temperature perception, and proprioceptive feedback to the surrounding tissues. Understanding this neuroanatomical foundation is crucial for comprehending why ear numbness occurs following facelift procedures and how the recovery process unfolds over time.
The sensory innervation of the auricular region involves multiple nerve branches originating from different anatomical sources. These neural pathways must be considered during surgical planning to minimise the risk of prolonged sensory deficits whilst achieving the desired aesthetic improvements. The complexity of this neural network explains why complete avoidance of temporary sensory changes remains challenging, even with the most meticulous surgical technique.
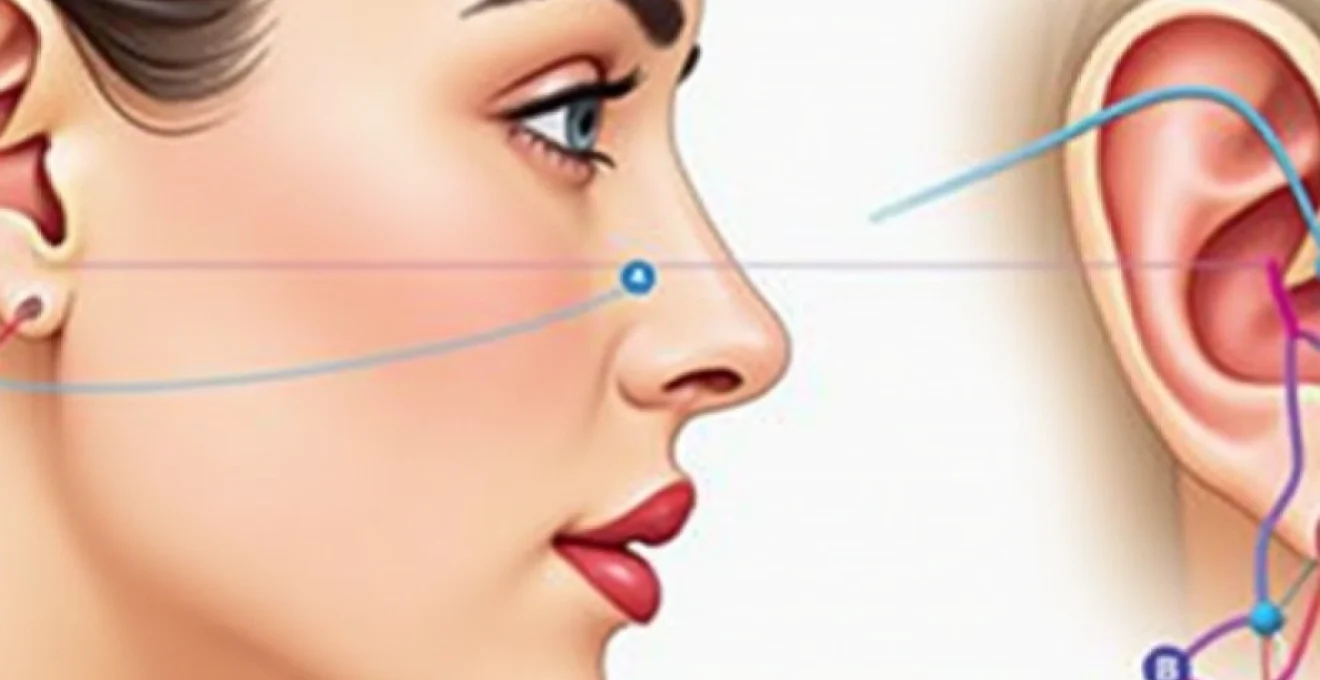
Greater auricular nerve anatomy and surgical vulnerability
The greater auricular nerve represents the most commonly affected neural structure during facelift surgery, originating from the cervical plexus at the C2-C3 spinal levels. This nerve travels anteriorly across the sternocleidomastoid muscle before dividing into anterior and posterior branches that supply sensation to the earlobe, external auditory canal, and adjacent facial skin. Its superficial course and proximity to standard facelift incision sites make it particularly vulnerable to surgical manipulation.
During deep plane facelifts or extensive SMAS (superficial musculoaponeurotic system) procedures, the greater auricular nerve may experience stretching, compression, or inadvertent trauma. The nerve’s relatively fixed position at its emergence point creates tension when facial tissues are mobilised and repositioned, leading to temporary neurapraxia in approximately 7-15% of patients undergoing comprehensive facial rejuvenation.
Cervical plexus distribution and facelift incision sites
The cervical plexus contributes multiple sensory branches that innervate the lower face, neck, and auricular regions. These include the lesser occipital nerve, greater auricular nerve, transverse cervical nerve, and supraclavicular nerves. The anatomical distribution of these neural pathways directly correlates with the typical incision patterns used in modern facelift techniques, creating inevitable proximity between surgical dissection planes and sensory innervation.
Surgical incisions extending from the temporal region, around the ear, and into the posterior hairline necessarily traverse multiple sensory territories. The overlapping innervation patterns explain why patients often experience numbness extending beyond the immediate surgical site, affecting areas such as the neck, jawline, and even portions of the scalp.
Sternocleidomastoid muscle relationship to auricular innervation
The sternocleidomastoid muscle serves as a crucial anatomical landmark during facelift surgery, with several important sensory nerves coursing along its surface. The greater auricular nerve emerges from beneath the posterior border of this muscle at Erb’s point, approximately 6.5 centimetres below the external auditory canal. This consistent anatomical relationship allows surgeons to identify and protect neural structures during dissection.
However, extensive mobilisation of cervical skin flaps and SMAS layers can create traction forces that affect nerves even when direct trauma is avoided.
The mechanical stress placed on neural tissues during tissue advancement and fixation can temporarily compromise nerve function, resulting in post-operative sensory changes that gradually resolve as inflammation subsides and normal tissue relationships are restored.
Temporal branch facial nerve considerations
Whilst primarily a motor nerve, the temporal branch of the facial nerve also carries some sensory fibres that contribute to auricular sensation. This nerve’s course through the temporal region makes it susceptible to injury during upper facelift procedures or temporal lifting techniques. Protecting this neural structure requires careful surgical technique and thorough understanding of its anatomical variations.
The temporal branch’s proximity to the superficial temporal artery and its course through the temporoparietal fascia create additional considerations during dissection. Inadvertent trauma to this nerve can result in both motor and sensory deficits , emphasising the importance of precise anatomical knowledge during surgical execution.
Immediate Post-Operative sensory changes following SMAS manipulation
The immediate post-operative period following facelift surgery is characterised by predictable patterns of sensory alteration that reflect the surgical trauma and inflammatory response. These changes typically manifest within hours of surgery completion and represent the body’s normal response to tissue manipulation and neural irritation.
Understanding the mechanisms behind immediate sensory changes helps patients distinguish between expected post-operative phenomena and potential complications requiring medical attention. The severity and distribution of initial numbness often correlate with the extent of surgical dissection and the specific techniques employed during the procedure.
Deep plane facelift impact on sensory pathways
Deep plane facelift techniques involve more extensive tissue mobilisation compared to superficial procedures, resulting in greater potential for sensory nerve involvement. This approach requires dissection beneath the SMAS layer, bringing surgical instruments into closer proximity with the facial nerve branches and associated sensory pathways. The increased tissue manipulation inherent in deep plane techniques often results in more pronounced initial numbness that may take longer to resolve.
The anatomical planes accessed during deep plane procedures contain numerous small sensory nerve branches that supply the overlying skin and subcutaneous tissues. Disruption of these neural networks creates areas of diminished sensation that gradually recover as nerve regeneration occurs and inflammatory processes subside. Patients undergoing deep plane techniques should anticipate potentially more extensive initial numbness compared to those receiving superficial facelift procedures.
Subcutaneous dissection effects on peripheral nerve function
Subcutaneous dissection during facelift surgery involves separation of skin and fat layers from underlying muscle and fascia, necessarily disrupting small cutaneous nerve branches that provide sensation to the overlying tissues. This process, whilst essential for achieving proper tissue mobilisation, inevitably results in temporary sensory deficits in the affected areas.
The extent of subcutaneous dissection directly correlates with the area of post-operative numbness. More aggressive skin undermining creates larger areas of sensory loss but may be necessary to achieve optimal aesthetic results. The trade-off between surgical access and temporary sensory changes represents a calculated decision based on individual patient anatomy and aesthetic goals.
Tumescent anaesthesia residual effects on sensation
Modern facelift procedures frequently employ tumescent anaesthesia techniques that involve infiltration of large volumes of dilute local anaesthetic solution into the surgical tissues. Whilst this approach provides excellent pain control and reduces bleeding, it can also contribute to prolonged sensory changes in the immediate post-operative period.
The residual effects of tumescent anaesthesia can mask the true extent of post-operative sensory changes for 12-24 hours following surgery.
As the anaesthetic effects gradually wear off, patients may notice evolving patterns of numbness and tingling that represent the underlying neural response to surgical trauma rather than continuing anaesthetic effects.
This temporal evolution of sensory symptoms is entirely normal and expected during the early recovery phase.
Post-surgical oedema and nerve compression mechanisms
Post-operative swelling represents one of the most significant factors contributing to early sensory changes following facelift surgery. The inflammatory response to surgical trauma results in tissue oedema that can compress sensory nerve branches, temporarily interfering with normal neural transmission. This compression-induced numbness often represents a larger component of immediate post-operative sensory loss than direct surgical trauma.
The relationship between oedema and sensory function explains why numbness often fluctuates during the early recovery period, correlating with changes in swelling patterns. As inflammation gradually resolves over the first several weeks, many patients notice corresponding improvements in sensation. This correlation between swelling reduction and sensory recovery provides reassurance that observed numbness is likely temporary rather than permanent.
Clinical assessment of auricular hypoesthesia Post-Rhytidectomy
Proper assessment of post-facelift sensory changes requires systematic evaluation using standardised testing protocols that can objectively quantify the degree and distribution of sensory loss. These assessment techniques allow surgeons to monitor recovery progress and identify patients who may require additional intervention or extended observation.
Clinical evaluation of auricular numbness extends beyond simple subjective reporting, incorporating objective measurements that can track improvement over time. This quantitative approach helps distinguish between normal recovery patterns and potential complications that might require specific treatment interventions.
Semmes-weinstein monofilament testing for sensory mapping
Semmes-Weinstein monofilament testing provides an objective method for assessing tactile sensation in specific anatomical regions affected by facelift surgery. This testing protocol uses calibrated nylon filaments of varying diameters to determine sensory thresholds at multiple anatomical points around the ears and adjacent facial areas.
The standardised nature of monofilament testing allows for precise documentation of sensory deficits and tracking of recovery progress over time. Normal auricular sensation typically corresponds to detection of 2.83 (0.07g force) monofilaments, whilst post-operative numbness may require 4.31 (2.0g force) or larger filaments for detection. Progressive improvement in monofilament detection thresholds provides objective evidence of neural recovery during the post-operative period.
Two-point discrimination assessment protocols
Two-point discrimination testing evaluates the ability to distinguish between two simultaneous tactile stimuli applied to adjacent skin areas. This assessment provides information about the functional quality of sensory recovery beyond simple touch detection thresholds. Normal auricular two-point discrimination typically ranges from 2-4 millimetres, depending on the specific anatomical location tested.
Post-operative changes in two-point discrimination often persist longer than basic touch sensation, reflecting the more complex neural processing required for this function. Recovery of normal discrimination abilities typically occurs gradually over 3-6 months following surgery, with some patients requiring up to 12 months for complete normalisation.
Quantitative sensory testing in Post-Facelift patients
Quantitative sensory testing (QST) encompasses a comprehensive battery of assessments including thermal sensation, vibration detection, and pressure sensitivity. These tests provide detailed characterisation of specific sensory modalities affected by facelift surgery and can identify subtle changes that might not be apparent through clinical examination alone.
QST protocols have revealed that different sensory modalities recover at varying rates following facial surgery. Thermal sensation often returns more slowly than mechanical sensation, whilst vibration detection may remain altered for extended periods.
This differential recovery pattern reflects the varying degrees of vulnerability among different types of sensory nerve fibres and their distinct regeneration characteristics.
Temporal progression of sensory recovery in facial rejuvenation surgery
The recovery of normal sensation following facelift surgery follows a predictable temporal pattern that helps patients understand what to expect during their healing journey. Most patients experience the greatest degree of numbness during the first 2-4 weeks post-operatively, with gradual improvement occurring over subsequent months. Understanding this timeline helps distinguish between normal recovery progression and situations that might require medical evaluation.
The initial phase of sensory recovery typically begins within the first month following surgery, characterised by the return of crude touch sensation and reduction in areas of complete numbness. This early improvement often coincides with resolution of post-operative swelling and reflects the recovery of neural function in areas where nerves experienced temporary dysfunction rather than actual damage. Patients frequently describe tingling sensations or altered sensitivity during this phase, which represents positive signs of neural regeneration.
The intermediate recovery phase, spanning months 2-6 post-operatively, involves refinement of sensory function and gradual normalisation of sensation quality. During this period, most patients notice significant improvement in their ability to perceive light touch, temperature changes, and tactile discrimination. However, some areas may continue to feel different from pre-operative sensation, with reports of hypersensitivity or altered sensation quality being common during this timeframe.
The final phase of sensory recovery extends from 6-12 months and sometimes beyond, involving the maturation of neural connections and achievement of stable sensory function. Whilst the majority of patients achieve near-complete sensory recovery during this timeframe, approximately 5-10% may experience some degree of permanent alteration in auricular sensation. These long-term changes are typically subtle and do not significantly impact daily function , though they may be noticeable to the patient during specific activities or when directly compared to the unaffected side.
Research studies tracking sensory recovery have demonstrated that 85-90% of patients achieve satisfactory return of auricular sensation within 6 months of surgery, with an additional 5-8% showing continued improvement up to 12 months. The remaining small percentage of patients may experience persistent mild numbness or altered sensation that remains stable beyond the one-year mark. Factors influencing recovery rates include patient age, surgical technique, extent of dissection, and individual healing characteristics.
Distinguishing transient neurapraxia from permanent nerve damage
Determining whether post-operative numbness represents temporary neural dysfunction or permanent damage requires careful clinical evaluation and understanding of distinct diagnostic criteria. Transient neurapraxia, the most common cause of post-facelift numbness, involves temporary disruption of nerve function without structural damage to the nerve itself. This condition typically resolves spontaneously as inflammation subsides and normal neural function is restored.
Clinical signs suggesting transient neurapraxia include gradual improvement in sensation over time, retention of some sensory function in affected areas, and absence of associated motor deficits or signs of infection. Patients with neurapraxia often report fluctuating sensory symptoms, with good days and bad days reflecting the dynamic nature of neural recovery. The progressive nature of improvement, even if slow, provides reassurance that permanent damage has likely not occurred.
Permanent nerve damage, whilst rare in modern facelift surgery, presents with distinct characteristics that differ from transient neurapraxia. These include complete absence of sensation in specific anatomical distributions, lack of improvement over extended time periods, and potential association with other neurological deficits.
Permanent sensory loss typically maintains consistent boundaries that correspond to specific nerve territories and does not show the fluctuating patterns characteristic of recovering neural function.
Diagnostic imaging studies, including high-resolution ultrasound or MRI, may occasionally be employed to evaluate suspected cases of significant nerve injury. However, these investigations are rarely necessary for routine post-facelift sensory changes and are typically reserved for cases with concerning clinical features or prolonged lack of improvement. Electrophysiological testing may also provide objective assessment of nerve function in selected cases where clinical evaluation alone is insufficient.
The timing of sensory recovery provides important diagnostic information, with complete absence of improvement beyond 12 months suggesting possible permanent change. However, case reports have documented continued sensory improvement up to 18-24 months following surgery in some patients, emphasising the importance of extended observation before concluding that changes are permanent. Individual variation in healing rates necessitates patient-specific evaluation rather than rigid adherence to standard timelines.
Evidence-based management strategies for Post-Facelift sensory deficits
Management of post-facelift ear numbness focuses primarily on patient education, symptom monitoring, and supportive care during the natural recovery process. Evidence-based approaches emphasise the temporary nature of most sensory changes whilst providing practical strategies to enhance patient comfort and potentially accelerate neural recovery. The foundation of effective management lies in setting appropriate expectations and providing ongoing support throughout the recovery journey.
Conservative management strategies form the cornerstone of post-facelift sensory care, with emphasis on protecting affected areas from inadvertent injury whilst sensation remains diminished. Patients are advised to avoid extreme temperatures, sharp objects, and excessive pressure on numb areas until normal sensation returns.
This protective approach prevents complications that could impair the healing process whilst allowing natural recovery mechanisms to proceed unimpeded.Gentle massage techniques may provide modest benefits in promoting circulation and potentially accelerating nerve regeneration, though evidence supporting these interventions remains limited. When recommended by the surgical team, light circular motions applied to areas adjacent to numb regions can stimulate blood flow without placing excessive stress on healing tissues. Patients should avoid direct pressure on incision sites and ensure that any massage techniques are performed according to specific post-operative instructions.Pharmacological interventions for post-facelift sensory deficits remain controversial, with limited evidence supporting their routine use. Some practitioners advocate for short-term corticosteroid administration to reduce inflammatory responses that may contribute to nerve compression, whilst others suggest vitamin B complex supplementation to support neural regeneration.
The risk-benefit profile of these interventions must be carefully considered on an individual basis, as potential side effects may outweigh modest therapeutic benefits in most cases.
Advanced therapeutic modalities, including low-level laser therapy and transcutaneous electrical nerve stimulation, have been investigated for post-surgical sensory recovery with mixed results. These treatments theoretically promote cellular metabolism and neural regeneration through photobiomodulation or electrical stimulation mechanisms. However, high-quality clinical trials demonstrating significant efficacy remain lacking, and such interventions should be considered experimental rather than standard care.Patient education represents perhaps the most crucial element of effective management, focusing on realistic timeline expectations and warning signs that might indicate complications requiring medical attention. Providing patients with written information describing normal recovery patterns helps reduce anxiety and unnecessary medical visits whilst ensuring appropriate follow-up when genuinely needed. Regular scheduled assessments allow for objective monitoring of progress and prompt identification of any concerning developments.The psychological impact of persistent numbness should not be underestimated, particularly when sensory changes exceed expected duration or severity. Some patients experience significant anxiety about permanent sensory loss, requiring additional support and reassurance throughout the recovery process. Cognitive-behavioral strategies and support group participation may benefit patients struggling with adaptation to temporary sensory changes, though such interventions are rarely necessary for routine post-facelift numbness.Surgical revision procedures for persistent sensory deficits are extremely rare and typically considered only in cases with documented permanent nerve injury affecting functional activities. These complex procedures carry significant risks and uncertain outcomes, making conservative management the preferred approach for the vast majority of patients experiencing post-facelift sensory changes. The decision to pursue surgical intervention requires careful multidisciplinary evaluation and extensive patient counselling regarding realistic expectations and potential complications.Long-term follow-up protocols should include systematic assessment of sensory recovery at predetermined intervals, typically at 6 weeks, 3 months, 6 months, and 12 months post-operatively. This structured approach enables early identification of atypical recovery patterns whilst providing reassurance for patients experiencing normal healing progression. Documentation of sensory changes using standardised assessment tools facilitates objective comparison over time and supports clinical decision-making regarding additional interventions.Research into novel therapeutic approaches for post-surgical sensory deficits continues to evolve, with investigations into growth factor therapies, stem cell applications, and advanced rehabilitation techniques showing preliminary promise. However, these experimental treatments remain in early developmental phases and are not yet appropriate for routine clinical application. The focus remains on optimising current evidence-based management strategies whilst continuing to refine surgical techniques that minimise the risk and severity of post-operative sensory disturbances.The integration of patient-reported outcome measures into routine post-facelift care provides valuable insights into the functional impact of sensory changes and the effectiveness of management interventions. These tools help quantify subjective experiences of numbness and track improvements in quality of life measures throughout the recovery process. Such comprehensive assessment approaches contribute to improved patient satisfaction and better understanding of factors influencing successful sensory recovery following facial rejuvenation surgery.